

Introduction
Due to the higher metabolic demand, malignant cells have an increased dependency on the nucleocytoplasmic trafficking of proteins, as compared to normal cells. Chromosome region maintenance protein 1 (CRM1), encoded by the XPO1 gene, is the main protein receptor which facilitates export of molecules, including tumor suppressor proteins, from the nucleus to the cytoplasm thereby making them inactive. Expression of CRM1 in tumor tissue has been shown to be an independent prognostic marker in several solid tumors and in acute myeloid leukemia; high CRM1 expression by immunohistochemistry (IHC) was associated with more aggressive disease and shorter survival. Importantly, selinexor, a first in class small molecule inhibitor of CRM1, was recently approved for the treatment of relapsed diffuse large B-cell lymphoma (DLBCL). The expression of CRM1 on tumor cells and the assessment of its prognostic impact have not been studied in patients (pts) with DLBCL or primary mediastinal B-cell lymphomas (PMBCL).
Methods
Paraffin embedded tumor tissue from pts with DLBCL or PMBCL treated with immunochemotherapy was assessed for CRM1 expression through IHC on tissue microarray (TMA). CRM1 anti-rabbit monoclonal antibody (Cell Signaling, catalog-no: 46249) was used at 1:100 dilution. Tumor cell grading was based on CRM1 staining in tumor cells compared to background non-malignant lymphocytes and non-malignant lymphocytes in spleen and tonsillar tissue controls. Renal cell carcinoma (RCC) was used as a positive control [known high levels of CRM1 staining (Inoue et al, J Urol, 2012)]. Two expert hematopathologists (RLK & AJW) independently scored CRM1 nuclear staining and assigned a grade of 0-3; 0 (no definitive nuclear staining, equal to background lymphocytes), 1 (dim nuclear staining), 2 (consistent nuclear staining, nuclear detail still visible behind the stain) and 3 (strong nuclear staining obscuring most nuclear detail, staining equivalent to RCC control). The average CRM1 score per case across all available cores on the TMA was calculated. Low CRM1 expression for a case was arbitrarily defined as a score of 0-2.0; high CRM1 expression was score 2.1-3.0. Scoring reliability between reviewers and between cores was assessed using intra-class correlation coefficient; score 0.75-0.90 was considered as a good scoring reliability. Event-free survival (EFS) was defined as time from diagnosis to progression, relapse, retreatment, or death. The association of CRM1 expression and risk of failing to achieve EFS at 24 months after diagnosis (EFS24) was estimated using odds ratios (OR) and 95% confidence intervals (CI) from logistic regression models, while the association of CRM1 expression with continuous EFS and overall survival (OS) was estimated using Kaplan-Meier curves and hazard ratios (HR) and 95% CI from Cox regression models.
Results
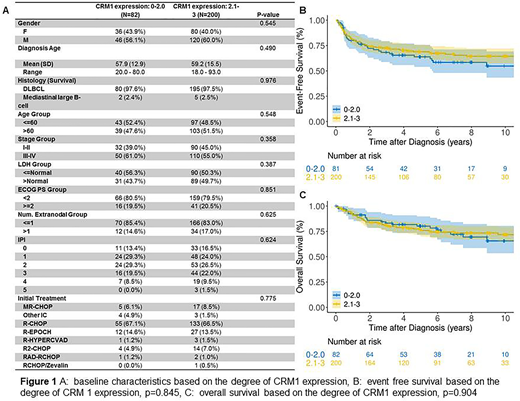
Tumor tissue from 282 pts was studied for CRM1 staining, including 275 pts with DLBCL and 7 pts with PMBCL. Median age of the study population was 61 years (range: 18-93) and 59% were male. The median follow-up for the entire cohort was 88.6 months. The first-line treatment regimens and baseline patient characteristics at diagnosis are outlined in Figure 1A. Of the 282 pts, 200 (71%) had high level of CRM1 expression and 82 (29%) had low CRM1 expression [only 4 (1.4%) had no or 0 staining]. Intra-class correlation coefficient to measure scoring reliability was 0.8. There was no difference in International Prognostic Index (IPI), ECOG performance score, lactate dehydrogenase or age at diagnosis among the groups with high CRM1 expression compared to low CRM1 expression (Figure 1A). The EFS24 failure was 29% for pts with low CRM1 expression while 26% in pts who had high CRM1 expression, OR=1.16, 95% CI 0.63-2.07; p=0.63. Null associations were also observed for EFS (HR=1.21, 95% CI 0.80-1.83; p=0.38) and OS (HR=1.02, 95% CI 0.61-1.69; p=0.95), (Figure 1B, C). Results were similar when adjusted for gender and IPI.
Conclusion
CRM1 expression by IHC on paraffin embedded tumor tissue is feasible in DLBCL and PMBCL. These data demonstrate that the CRM1 protein, the target for selinexor, is indeed expressed in the vast majority of these tumors; only 1.4% had no staining. However, CRM1 expression by IHC is not a prognostic marker for EFS24, EFS or OS. Whether CRM1 staining predicts selinexor response has not been studied but should be included in any new studies using CRM1 inhibitors.
Maurer:Nanostring: Research Funding; Morphosys: Membership on an entity's Board of Directors or advisory committees; Pfizer: Membership on an entity's Board of Directors or advisory committees; Kite: Membership on an entity's Board of Directors or advisory committees; Celgene / BMS: Research Funding. Cerhan:BMS/Celgene: Research Funding; NanoString: Research Funding. Witzig:Acerta: Research Funding; Immune Design: Research Funding; Incyte: Consultancy; MorphSys: Consultancy; Celgene: Consultancy, Research Funding; Spectrum: Consultancy; Karyopharm Therapeutics: Research Funding; AbbVie: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal